Story by Connor Danielowski / May 29, 2026

Unlock recurring practice income with Chronic Care Management. Learn how a 1,000-patient CCM panel stabilizes revenue and meets CPT 99490 requirements effectively.

Most practices are trapped on a fee-for-service hamster wheel – revenue stops the moment a physician stops seeing patients.
The solution isn’t seeing more patients. It’s getting paid for the care that already happens between visits.
Traditional revenue model constraints are straightforward: a physician has roughly 20–22 billable patient slots per day, and that ceiling doesn’t move. No matter how efficiently a practice operates, income is forever tethered to hours worked. Overhead climbs, staffing costs rise, and the math never quite improves.
Chronic Care Management changes that equation entirely. Defined by CMS as a billable service covering non-face-to-face care coordination for patients with two or more chronic conditions, CCM reimbursement under CPT code 99490 is paid for the work of qualified clinical staff – not exclusively physician time. A trained care coordinator makes the calls, updates the care plan, and coordinates referrals. The physician supervises but isn’t the one clocking every minute. That structural shift is what makes CCM feel less like a procedure code and more like a subscription model – recurring practice income attached to an enrolled patient panel rather than to appointment slots.
The 1,000-patient panel is where the math becomes impossible to ignore. Below that threshold, CCM is a useful supplement. At or above it, CCM revenue becomes a genuine financial stabilizer – predictable, scalable revenue running parallel to your existing practice income. Understanding which patients qualify is the first operational step toward building that panel deliberately.
The next question is simple: what does 1,000 enrolled patients actually generate each month?
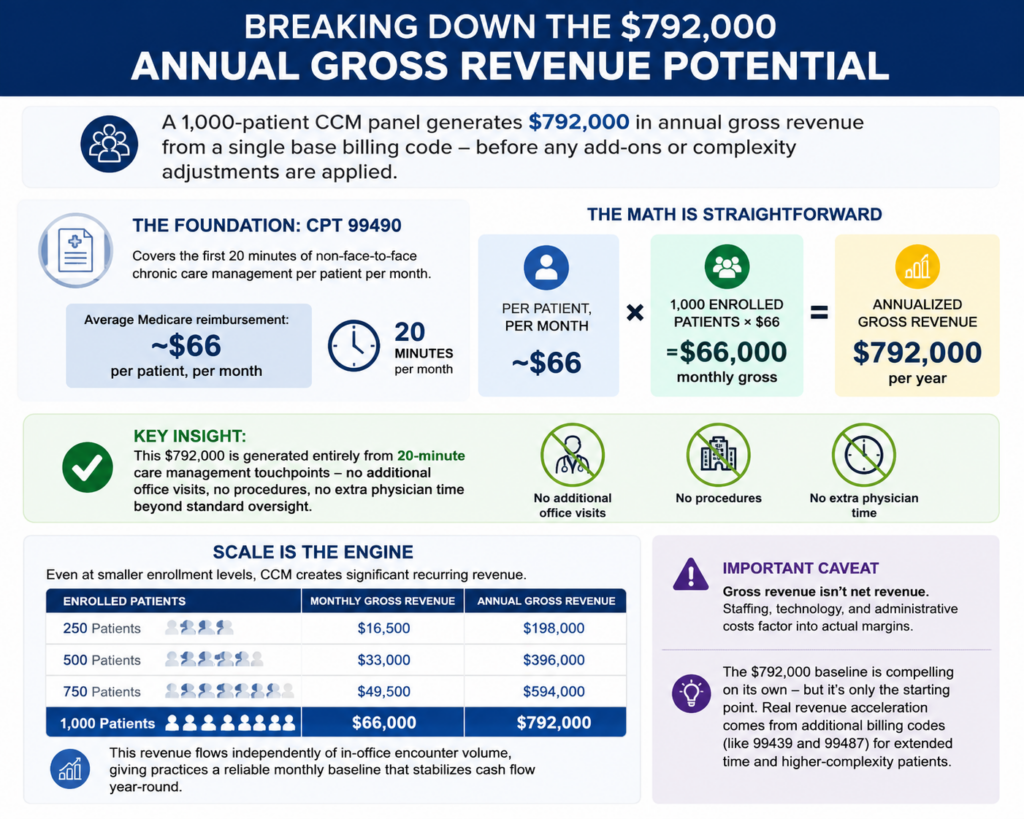
A 1,000-patient CCM panel generates $792,000 in annual gross revenue from a single base billing code – before any add-ons or complexity adjustments are applied.
The foundation of all CCM revenue is CPT 99490, which covers the first 20 minutes of non-face-to-face chronic care management per patient per month. According to Chronic Care Staffing research, the national average Medicare reimbursement for this code is approximately $66 per patient per month. That figure may seem modest in isolation, but it scales powerfully across a full panel.
The math is straightforward:
Key insight: This $792,000 is generated entirely from 20-minute care management touchpoints – no additional office visits, no procedures, no extra physician time beyond standard oversight.
Scale is the engine here. A practice enrolling even 500 patients captures $396,000 annually from the base code alone. As noted in the previous section, this revenue flows independently of in-office encounter volume, giving practices a reliable monthly baseline that stabilizes cash flow regardless of appointment fluctuations or seasonal slowdowns.
One important caveat: gross revenue isn’t net revenue. Staffing, technology, and administrative costs factor into actual margins. However, understanding how CCM works at a structural level makes clear why even conservative enrollment targets produce a meaningful financial floor.
The $792,000 baseline is compelling on its own – but it’s only the starting point. The real revenue acceleration comes from the additional billing codes that layer on top of 99490 for extended time and higher-complexity patients.

The $792,000 baseline figure is compelling – but Chronic Care Management ROI increases significantly higher once add-on and complexity codes enter the picture.
The base CPT 99490 code covers the first 20 minutes of monthly care, but many patients routinely require more time. That’s where the billing structure rewards thoroughness.
Key codes that expand your panel’s revenue ceiling:
In practice, a realistic panel isn’t monolithic. Patient acuity varies. A common planning assumption is that roughly 20% of a 1,000-patient panel will qualify for complex CCM billing in any given month. Run the numbers on that cohort alone, and the incremental gain exceeds $122,400 in additional annual revenue – on top of the base panel income.
That compounding effect is exactly why building a structured CCM and RPM workflow matters from day one. Accurate time tracking, documented care plan complexity, and consistent monthly outreach aren’t just compliance requirements – they’re the operational levers that determine whether your practice captures the full multiplier or leaves money on the table.
However, complexity billing requires careful documentation. Unsupported claims invite audit risk, so clinical rigor must match billing ambition.
This same patient-level attention also creates a natural opening for another high-value revenue stream – one driven almost entirely by the touchpoints CCM already establishes.
CCM creates a powerful secondary revenue stream by positioning care managers as the natural scheduling engine for high-value Medicare care coordination revenue.
The overlooked connection: Patients who meet CPT 99490 requirements for billing – two or more chronic conditions with expected duration of 12 months or more – are precisely the patients who most benefit from, and most frequently miss, their Annual Wellness Visit. Regular monthly touchpoints give CCM care managers a consistent, low-friction opportunity to identify AWV-eligible patients and get them scheduled before the calendar year closes.
According to THA.org, CCM enrollment is the perfect touchpoint to schedule Annual Wellness Visits. That alignment is no accident. The AWV structure itself – built around a Health Risk Assessment and chronic condition review – mirrors the ongoing care planning that CCM coordinators already perform. The conversation flows naturally.
The financial upside is significant. AWV codes G0438 (initial visit) and G0439 (subsequent visit) each reimburse in the range of $170 per visit under Medicare. Across a 1,000-patient panel, even a 70% AWV capture rate generates roughly $119,000 in additional annual income. At full utilization – 1,000 completed visits – that figure climbs past $170,000 per year.
In practice, practices without a structured CCM program routinely leave AWV revenue on the table simply because no one is tracking eligibility or following up. Care managers change that dynamic. They hold the patient relationship between visits, which means they are the most effective resource for closing preventive care gaps that billing teams rarely have time to chase.
Of course, capturing this revenue requires the right staffing infrastructure – which raises an important question about what it actually costs to run a 1,000-patient panel at this level.
Recurring practice income from CCM is real – but so are the costs, and understanding both sides of the ledger is what separates sustainable programs from short-lived ones.
The staffing math is straightforward: a 1,000-patient panel typically requires 3 to 4 full-time Care Managers. This benchmark follows the widely recommended 1:250 care manager-to-patient ratio, which ensures each patient receives the minimum 20 minutes of monthly contact time required for billable CCM – without burning out staff or compromising documentation quality.
Labor is by far the largest line item. Factoring in salaries, payroll taxes, and benefits, four full-time Care Managers will cost a practice roughly $280,000 annually. That number can shift depending on geography and whether staff are hired directly or sourced through a remote CCM staffing model, which can reduce overhead associated with physical office space and HR administration.
Software and platform fees are comparatively modest. Expect to pay approximately $5 per patient per month for a compliant CCM platform that handles time-tracking, care plan documentation, and monthly billing exports. For a 1,000-patient panel, that totals roughly $60,000 per year – a predictable, scalable cost.
Stacking those figures together:
Against the $792,000 gross revenue baseline discussed earlier, that leaves an estimated net profit of approximately $452,000 per year, according to Chronic Care Staffing’s internal analysis. Of course, actual margins will vary based on your payer mix, enrollment rate, and staff efficiency.
Those operational returns are compelling on their own – but CCM’s financial impact extends well beyond the billing statement, particularly when you factor in what strong CCM infrastructure does for your performance scores and value-based contracts.
CCM is one of the most efficient tools a practice can deploy to strengthen its position under value-based reimbursement – converting routine care coordination into measurable financial protection.
MIPS performance directly determines whether Medicare pays you more or less. The Merit-based Incentive Payment System evaluates practices across four categories, and CCM activity feeds two of the most weighted: Clinical Care and Care Coordination. Documenting monthly touchpoints, medication reviews, and care plan updates generates the clinical data that MIPS auditors look for. A well-run CCM program can push a practice’s composite score high enough to unlock a positive payment adjustment – currently up to 9% – while practices that fall below the performance threshold face a penalty of equal magnitude. That 18-point swing in Medicare care coordination revenue is material for any practice with a significant Medicare panel.
The shared savings upside is equally compelling for ACO participants. Per CMS evaluation data, CCM identifies issues before they escalate into ER visits – which directly reduces total cost of care, the core metric that determines shared savings distributions. Fewer hospitalizations mean a lower per-member expenditure versus benchmark, and that gap translates into bonus payments flowing back to the practice. The evidence on reduced ER utilization reinforces why ACO administrators increasingly view CCM enrollment as a non-negotiable infrastructure investment, not an optional add-on.
On the other hand, capturing these gains requires consistent execution – which brings a critical operational question into focus: who actually does the work? Whether a practice builds that capacity internally or looks to an external solution is a decision with significant financial and strategic consequences.

Choosing how to staff a CCM program is often the single decision that determines whether the revenue opportunity ever becomes real.
In-house programs offer appealing control – your care managers know your patients, your EHR, and your protocols. In practice, however, that control comes at a steep price. Recruiting qualified clinical staff is competitive, onboarding takes months, and turnover can collapse an enrollment pipeline overnight. Every vacancy means patients go un-enrolled, and un-enrolled patients mean forfeited reimbursement.
The math on this is sobering. According to a Star Gazette press release, most primary care practices are missing up to $647,000 a year in Medicare revenue – largely because they lack the dedicated staffing infrastructure to run CCM at scale. That gap is not a billing problem. It is a capacity problem.
Outsourced staffing addresses that capacity problem directly. A turnkey model means trained care managers, documented workflows, and compliance infrastructure are already in place – without the HR overhead of recruiting, benefits administration, or coverage gaps. For practices that have already reviewed who qualifies for the program and confirmed a large eligible panel, outsourcing compresses the time from decision to revenue significantly.
The comparison breaks down like this:
The cost of missed enrollment almost always outweighs the cost of outsourcing. A practice sitting on 800 eligible patients but enrolling only 200 is leaving more on the table than any vendor fee could represent.
With the staffing model clarified, the full financial picture of the 1,000-patient panel comes into sharp focus.
A fully enrolled 1,000-patient CCM panel is one of the few revenue models in primary care that scales without demanding more of the physician’s time.
Here’s what the numbers look like when the model runs at full capacity:
The single most important shift this model creates is structural independence from the exam room.
That distinction matters enormously in a landscape where physician burnout, staffing shortages, and payer pressure are compressing traditional fee-for-service margins. As MGMA has noted, CCM represents one of the most underleveraged revenue opportunities available to practices today – and the financial case only strengthens when you factor in the broader clinical and financial advantages that accrue over time.
What You Need to Know: A 1,000-patient CCM panel can realistically generate $400,000–$500,000 in net annual income, reduce dependence on physician volume, and create durable revenue through value-based incentives – but only if the staffing model is right from the start. That’s exactly where the next step begins.
The fastest path to capturing CCM revenue is a structured audit of your existing patient data – the opportunity is already sitting in your EHR.
Start with a simple report: Pull every patient with two or more documented chronic conditions who carries Medicare Part B coverage. This single query typically surfaces 20–40% of an average primary care panel as CCM-eligible, a number that surprises most practice administrators. Per CMS Billing Guidelines, each enrolled patient also requires documented verbal or written consent and a completed care plan – so flag those workflow steps early.
Next, assess your staffing reality honestly. Compare your current clinical staff capacity against the 1:250 nurse-to-patient ratio that a sustainable CCM program demands. If your team is already stretched across appointment scheduling, prior authorizations, and in-office care, adding 20-minute monthly CCM touchpoints without dedicated support will stall enrollment before it scales.
Then decide how to launch:
The $792,000 revenue opportunity is real, but it’s not passive. A 1,000-patient CCM panel becomes a practice stabilizer only when the enrollment engine is running. Audit your panel this week, identify your staffing gap, and take the first step toward a sustainable, scalable revenue model built around the patients you already serve.