Story by Connor Danielowski / June 1, 2026

Break free from the fee-for-service trap. Learn how Chronic Care Management creates a sustainable, subscription-based revenue model for your medical practice.

Most medical practices are running on a treadmill – and the moment the doctor steps off, the revenue stops. That’s the defining vulnerability of the traditional fee-for-service model, where income is entirely tied to in-person, episodic encounters.
A practice that bills only for sick visits is one slow month – or one physician absence – away from a cash flow crisis.
In practice, this volatility is compounded by how most clinics handle revenue cycle management. According to the MGMA’s Revenue Cycle Management guidance, traditional RCM is often viewed as a back-office function rather than a strategic growth lever – reactive by design, chasing reimbursements rather than engineering them.
The shift toward intelligent RCM changes that calculus. Instead of billing for isolated encounters, forward-thinking practices are prioritizing longitudinal care – ongoing patient relationships that generate predictable, monthly reimbursement. This is what recurring revenue looks like in a clinical context: structured payments for continuous management of patients living with chronic conditions, regardless of whether an office visit occurred.
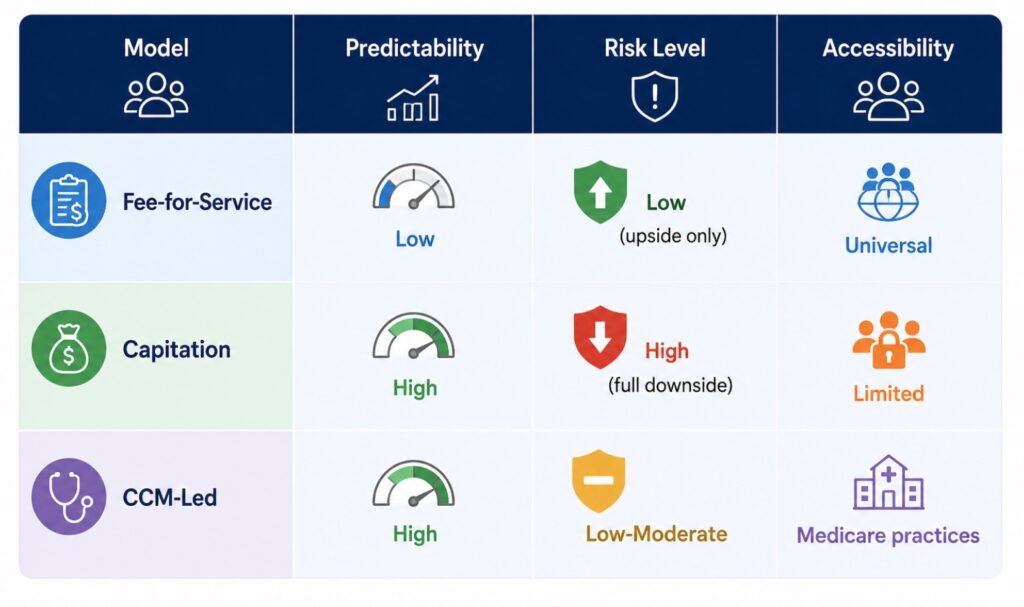
The debate around capitation vs. fee-for-service has long framed this as an either/or choice. However, a smarter middle ground exists – and understanding it starts with how recurring revenue models actually work inside today’s Medicare framework.
Not every recurring revenue model fits every practice – and the gap between what sounds strategic and what’s actually implementable is where most small practices get stuck.
Capitation offers predictable monthly payments, but it transfers full financial risk to the provider. If patient utilization spikes, the practice absorbs the loss. For independent or small group practices without actuarial infrastructure, that downside exposure is genuinely dangerous.
Direct Primary Care (DPC) and the broader subscription-based healthcare model solve the predictability problem elegantly – but at a cost. Panels are intentionally small, monthly membership fees replace insurance billing, and the economics depend on a patient base with disposable income. In FQHC settings or underserved communities, that model often simply doesn’t work.
The fundamental shift from “selling units” to “managing outcomes” over time is what makes recurring revenue durable – but most practices need a path that doesn’t require rebuilding their entire operating model.
That path is CCM. Operating entirely within the existing Medicare billing framework, Chronic Care Management functions as a synthetic subscription-based model – monthly, per-patient, and billable without capitation risk. Practices capture the financial structure of value-based care reimbursement without accepting full downside accountability.
That accessibility is precisely why CCM deserves a closer look at the actual revenue math – which is where most practices are genuinely surprised.
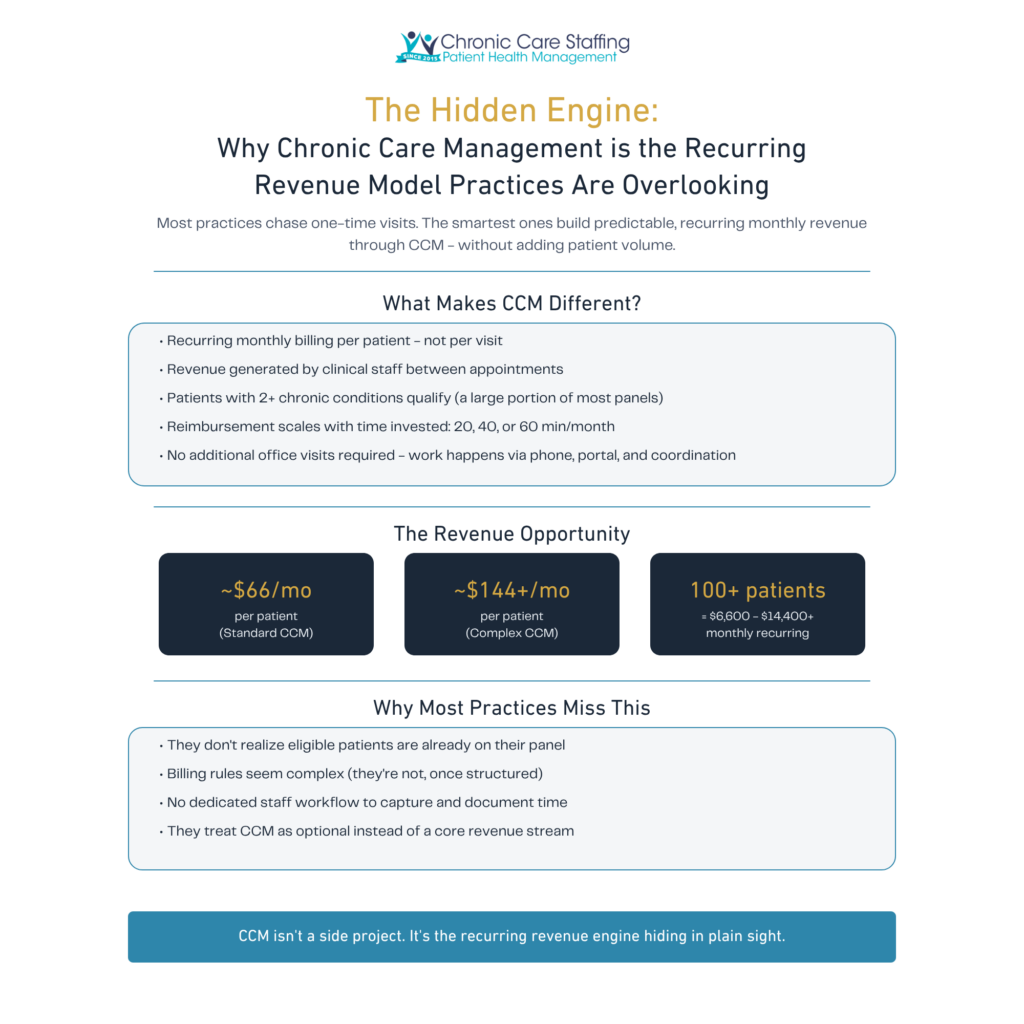
Chronic Care Management is the clearest example of a recurring revenue model most practices are sitting on – and systematically ignoring. Unlike unpredictable procedure volume or seasonal wellness visits, CCM generates billable revenue every single month for patients who are already in your care.
The math is straightforward. A practice with 500 eligible Medicare patients enrolled in CCM – billed at approximately $66 per patient per month under CPT 99490 – generates roughly $33,000 monthly, or over $396,000 annually. That’s predictable, recurring income that doesn’t fluctuate with flu season or vacation scheduling.
“CCM revenue doesn’t just improve cash flow – it fundamentally changes how a practice is valued by lenders, acquirers, and partners.”
Net revenue forecasting becomes dramatically more reliable when a monthly CCM baseline replaces volatile fee-for-service cycles. Practices exploring a direct primary care business model often cite this predictability as the deciding factor.
The longer-term upside is equally significant. The structured patient data CCM generates – documented care plans, monthly engagement records, outcome tracking – creates exactly the kind of longitudinal dataset that qualifies practices for higher-tier value-based contracts. You can explore how a structured CCM program builds that foundation systematically.
The revenue potential is real. The operational challenge of actually capturing it is where many practices stumble.
Knowing CCM exists and actually running it are two entirely different problems – and the gap between them is where most practices quietly give up.
The staffing paradox is the first wall practices hit. You need consistent monthly revenue to justify hiring a dedicated care coordinator, but you need that coordinator to generate the monthly CCM revenue in the first place. Without a clear path through this chicken-and-egg problem, most practices default to assigning CCM tasks to whoever has a free moment – which predictably means no one does it consistently.
Inefficiencies in the revenue cycle often stem from a lack of dedicated resources for non-face-to-face care coordination, and that resource gap compounds fast. The three operational bottlenecks that derail even well-intentioned programs are:
In practice, these bottlenecks don’t appear individually – they pile up simultaneously. Solving them requires more than goodwill; it requires a dedicated operational structure. That’s exactly what the next section addresses.

The fastest way to build a model of recurring revenue with Chronic Care Management (CCM) is to staff it correctly from day one – because the program lives or dies on consistent, compliant patient outreach.
Specialized clinical staff aren’t a support function – they are the revenue engine itself.
The outsourcing vs. in-house question is where most practice leaders stall. In-house staffing offers control but demands hiring, training, and compliance oversight that competes directly with existing team bandwidth. A turnkey CCM partner, by contrast, arrives with trained staff, established workflows, and CMS-aligned documentation protocols already in place. As the AHA’s framework for intelligent RCM makes clear, sustainable results require integrating clinical workflows with financial goals so no patient falls through the cracks – something a dedicated external team is structurally built to do.
The critical gap most practices underestimate is the distance between holding a billable CPT code and running an actual program. Having the code means nothing without staff making monthly contact, logging compliant minutes, and coordinating care plans. A specialized staffing partner like Chronic Care Staffing bridges exactly that gap, handling the clinical labor while your business office focuses on growth and patient acquisition.
The practical outcome: clinical quality stays high, billing stays consistent, and physician capacity stays protected – the foundation every practice leader needs to consider before the final numbers come into focus.
The opportunity inside your existing panel is almost certainly larger than you think – and a simple audit can reveal it in under a week.
Building a recurring revenue model with CCM starts with one practical first step: identifying the right patients. Pull your Medicare and Medicaid panel, filter for patients carrying two or more chronic diagnoses, and cross-reference against those who’ve had at least one office visit in the past 12 months. That list is your CCM-eligible population – and for most primary care practices, it’s substantial.
Don’t wait for perfect conditions. Value-based care transformation is a moving target. Practices that delay CCM enrollment while watching for “optimal” reimbursement structures consistently leave predictable monthly revenue unclaimed. A 30-day implementation goal is realistic: identify your eligible patients, enroll and obtain consent, and begin billing in month one.
In practice, the details of compliance, staffing, and workflow design can slow even motivated teams. That’s where external clinical support removes friction – handling the operational complexity so your providers focus on care.
Chronic Care Management is already working inside practices like yours. The question isn’t whether to start – it’s how soon. Connect with Chronic Care Staffing for a clinical and financial assessment tailored to your panel.
