Story by Connor Danielowski / May 28, 2026
Stop leaving revenue on the table. Learn how to optimize billing for CPT codes 99490, 99439, and 99487 to increase your practice’s Medicare CCM reimbursement.
Most practices are leaving hundreds of dollars per patient on the table every month – not through billing errors, but through stopping too soon.
The 99490 CPT code description is straightforward: per CMS MLN909188, it covers the first 20 minutes of clinical staff time per calendar month directed by a physician or qualified health care professional for patients with two or more chronic conditions. That 20-minute threshold is the entry point – not the ceiling.
Clinical labor is a billable asset. Medicare’s shift away from episodic, in-office visits toward continuous chronic disease management means the minutes your clinical staff spend on care coordination, medication reconciliation, and patient outreach are reimbursable. Many practices recognize this when scheduling an annual wellness visit but overlook it entirely during the months in between.
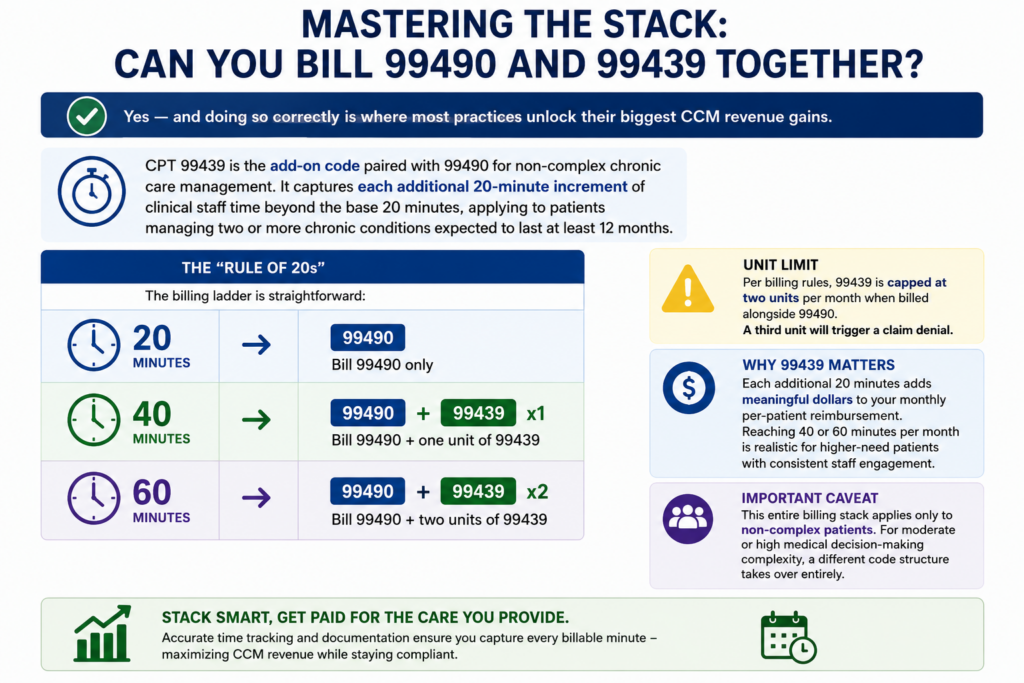
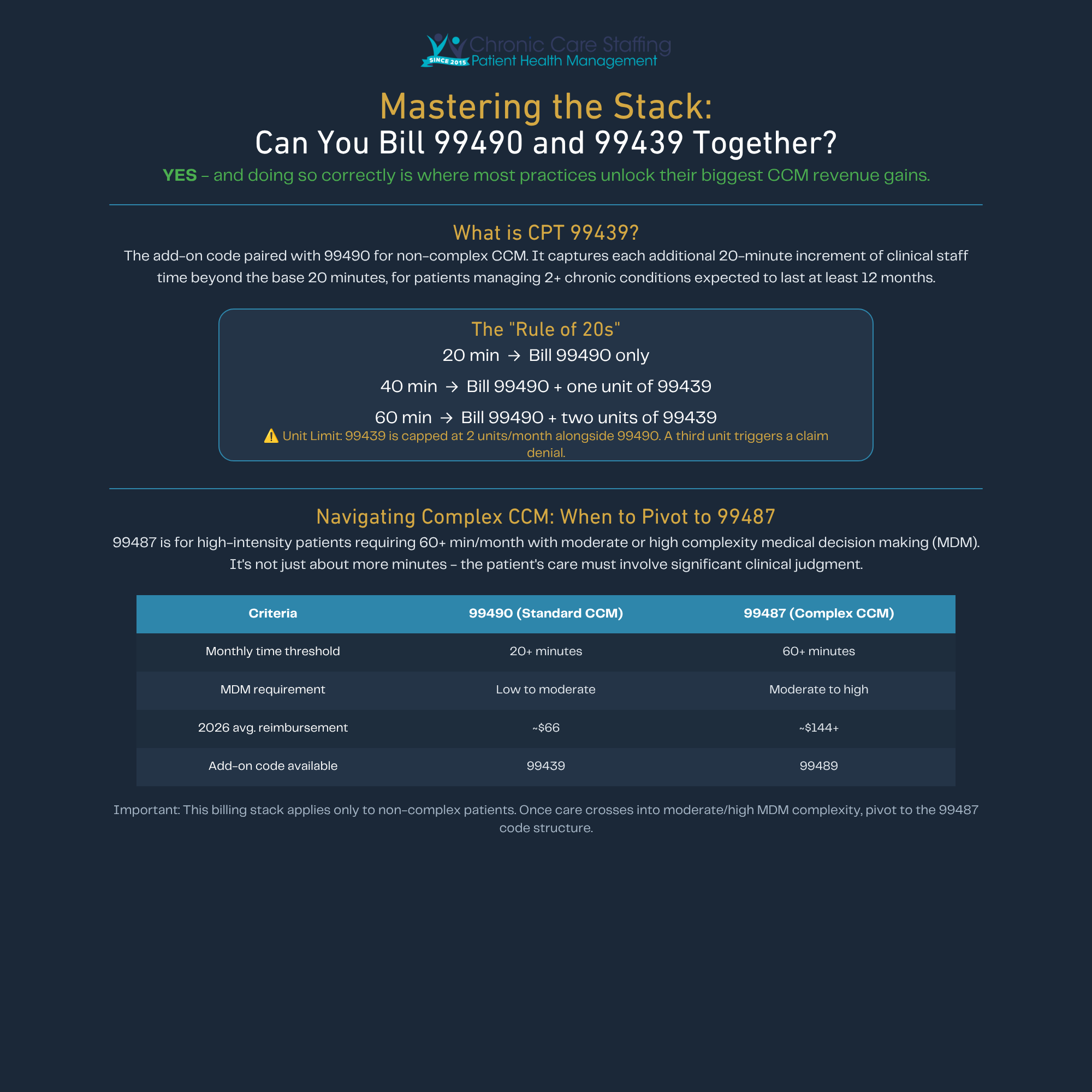
Yes – and doing so correctly is where most practices unlock their biggest CCM revenue gains.
CPT 99439 is the add-on code paired with 99490 for non-complex chronic care management. It captures each additional 20-minute increment of clinical staff time beyond the base 20 minutes, applying to patients managing two or more chronic conditions expected to last at least 12 months.
The “Rule of 20s” makes the billing ladder straightforward:
Unit limit: Per Chronic Care Staffing’s billing rules, 99439 is capped at two units per month when billed alongside 99490. Attempting a third unit will trigger a claim denial.
Understanding 99439 reimbursement matters because those additional units aren’t trivial – each adds meaningful dollars to the monthly per-patient total covered in the previous section. In practice, reaching 40 or 60 minutes per month is realistic for higher-need patients, especially when clinical staff are systematically engaged between visits.
One important caveat: this entire billing stack applies only to non-complex patients. Once a patient’s care crosses into moderate or high medical decision-making complexity, a different code structure takes over entirely – which is exactly where the next section picks up.

Not every chronic care patient needs the same level of management – and billing as if they do means leaving real money unclaimed.
The 99487 cpt code is designed for high-intensity patients who require at least 60 minutes of clinical staff time per month, paired with moderate or high complexity medical decision making (MDM). That MDM requirement is the critical differentiator. It’s not simply about clocking more minutes – the patient’s care must involve multiple chronic conditions with significant risk, prescription drug management, or decisions that would challenge straightforward clinical judgment.
Here’s how 99490 and 99487 compare side by side:
| Criteria | 99490 (Standard CCM) | 99487 (Complex CCM) |
|---|---|---|
| Monthly time threshold | 20+ minutes | 60+ minutes |
| MDM requirement | Low to moderate | Moderate to high complexity |
| 2026 avg. reimbursement | ~$66 | ~$144+ |
| Add-on code available | 99439 | 99489 |
The documentation burden for 99487 is substantially higher. Practices must demonstrate not just time, but the clinical reasoning that justifies complex-level care – typically through detailed care plan notes and documented decision points.
In practice, under-billing 99487-eligible patients as 99490 is one of the most common – and costly – CCM coding errors. A patient with uncontrolled diabetes, CHF, and CKD almost certainly qualifies. Recognizing that distinction early often means the difference between capturing $66 or $144 per patient, per month.
Identifying which patients qualify for 99487 often starts well before the monthly care management clock begins – which is where structured enrollment touchpoints, like the annual wellness visit, become essential.

The Annual Wellness Visit is one of the most underutilized entry points for CCM enrollment – and pairing it with a structured consent workflow directly accelerates CCM medicare reimbursement for your practice.
The AWV is a primary initiating visit where providers establish the comprehensive care plan required to bill CCM. The billing synergy is straightforward: G0438 (initial AWV) or G0439 (subsequent AWV) reimburses separately while simultaneously creating the clinical foundation for CCM activation. One visit, two revenue streams.
The process flow looks like this:
Proper documentation isn’t just good practice – it’s the frontline defense that keeps your ccm cpt codes claims standing during a Medicare audit.
The biggest compliance mistakes are almost always preventable. Watch for these audit red flags:
“Practices must use a certified EHR to report CCM, and the care plan must be available electronically 24/7 to all care providers.”
EHR compliance also means that every care team member – regardless of location – can access the patient’s current plan. This is especially relevant for patients managing multiple chronic conditions who may see multiple providers across different settings.
The clinical labor bottleneck is the single biggest obstacle between a practice and consistent medicare ccm reimbursement. Most practices simply don’t have staff available to log 20+ minutes of documented, billable time per patient every month – and hiring internal care coordinators adds salary, benefits, and training overhead that quickly erodes the revenue gain.
Outsourced staffing models solve this directly. Chronic Care Staffing provides the clinical personnel required to meet CCM time requirements without increasing practice overhead – handling time-tracking, care plan documentation, and patient outreach so your internal team stays focused on in-office care.
The ROI comparison is straightforward:
In practice, the outsourced approach scales as your patient panel grows – no hiring lag, no coverage gaps. Practices pursuing a value-based care strategy also find that outsourced CCM staffing accelerates quality metric performance alongside revenue.
Focus on your patients. Let the experts manage the documentation, time-logging, and billing hierarchy that turns chronic care into sustainable practice revenue.
