Story by Connor Danielowski / June 3, 2026
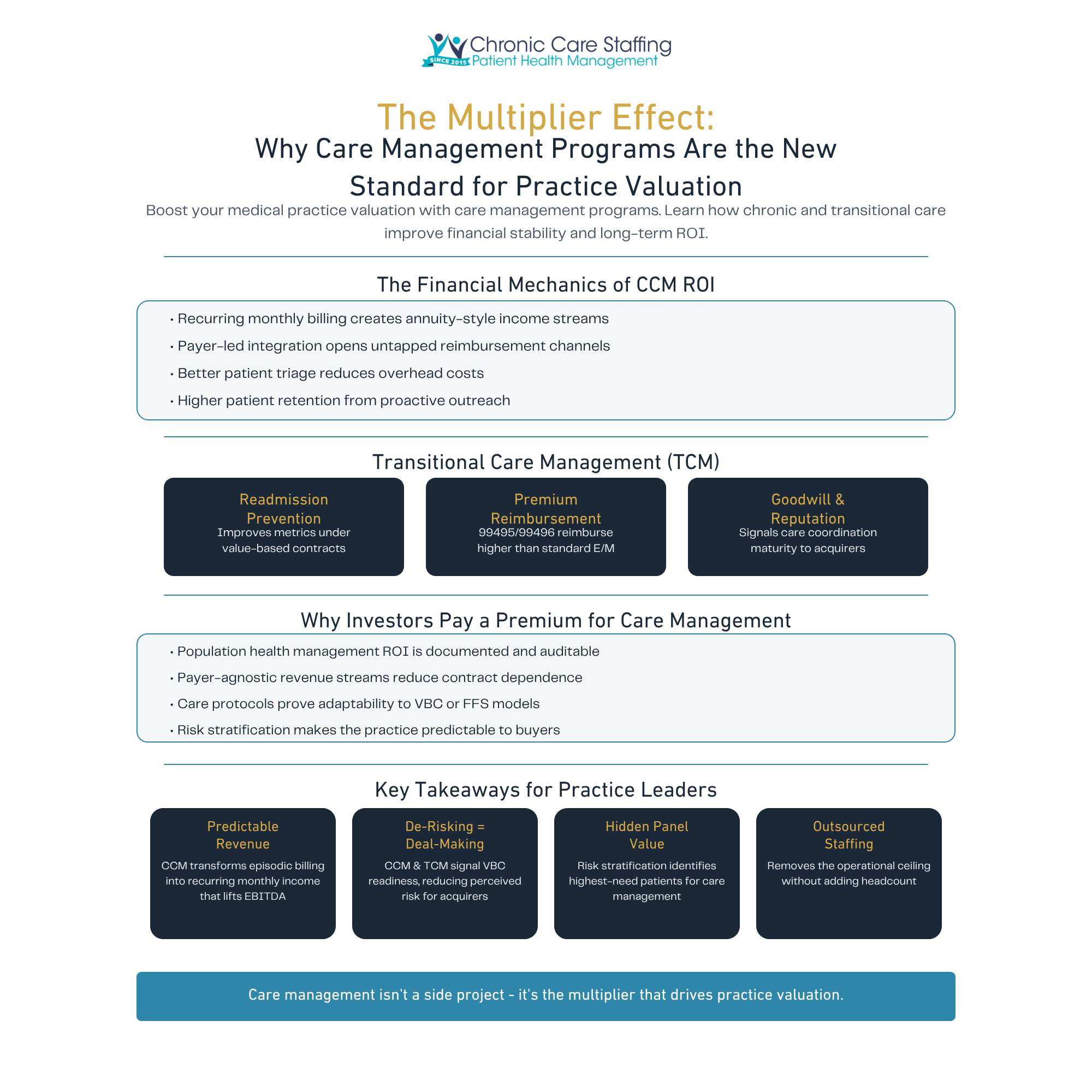
Boost your medical practice valuation with care management programs. Learn how chronic and transitional care improve financial stability and long-term ROI.
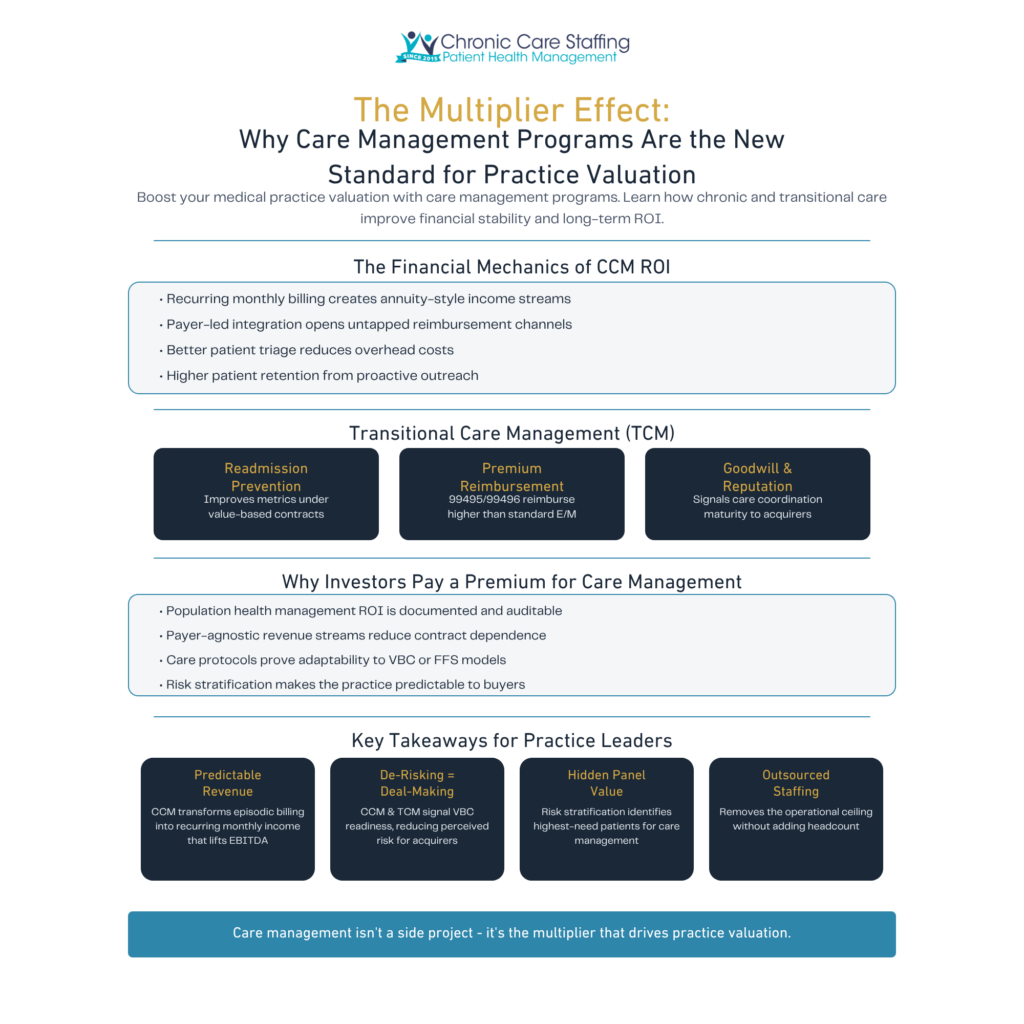
Chronic Care Management (CCM) programs generate recurring, predictable revenue that fundamentally changes how a practice’s financial health is measured and valued.
Unlike one-time procedure billing, CCM reimbursement operates on a monthly cycle. CMS reimburses CPT code 99490 for at least 20 minutes of non-face-to-face care coordination per month, with complex CCM codes unlocking higher reimbursement tiers.
The revenue drivers stack meaningfully:
Understanding how CCM works in practice clarifies why these revenue streams are so durable: the care model itself incentivizes continuity.
CCM’s real margin impact isn’t just top-line revenue growth — it’s the simultaneous reduction of overhead costs that makes it a rare double-sided driver of practice profitability.
That foundation of consistent, measurable engagement also sets the stage for one of CCM’s most powerful downstream benefits: protecting revenue during the riskiest gaps in patient care.

Transitional Care Management (TCM) is one of the highest-leverage tools a practice can deploy — both for patient outcomes and for demonstrating financial discipline to prospective buyers.
Transitional care management (TCM): TCM refers to structured clinical support provided to patients during the 30 days following discharge from a hospital, skilled nursing facility, or other inpatient setting. As the AAFP Value-Based Care Guide notes, this post-acute window carries the highest risk for costly readmissions and preventable complications.
The financial impact of a strong TCM program hits on three distinct levels:
A practice that controls the post-discharge gap controls one of the most expensive moments in a patient’s care journey. That operational discipline doesn’t go unnoticed during due diligence — and it connects directly to why investors place a valuation premium on practices with proven care management infrastructure, a point the next section explores in depth.

Practices with mature care management programs are fundamentally lower-risk investments — and private equity due diligence teams are increasingly pricing that reality into their valuations.
Risk stratification is the process of categorizing patients by clinical complexity and cost potential. For a PE team, a practice that already stratifies its population isn’t just clinically sophisticated — it’s predictable. Predictability compresses risk, and compressed risk justifies a higher multiple.
“Care management is the clinical engine of value-based care, providing the infrastructure for risk-sharing success.” — Baylor College of Medicine Executive Summary
The data generated through care management also functions as a Health IT Playbook for scalability. Structured workflows, documented outcomes, and utilization patterns give acquirers a replicable operational template — not a black box.
De-risking Factors investors identify in care management-mature practices:
A practice that succeeds in care management has already proven it can operate under accountability — the defining trait of any value-based care model.
Ultimately, care management isn’t just a revenue line — it’s organizational proof. The real question then becomes: who delivers that care consistently enough to sustain the premium?
Staffing is the single most decisive factor in whether a care management program generates consistent revenue — or quietly stalls out before it ever moves the needle on financial metrics for medical practices.
The build-vs-buy decision is straightforward when you map it against valuation impact:
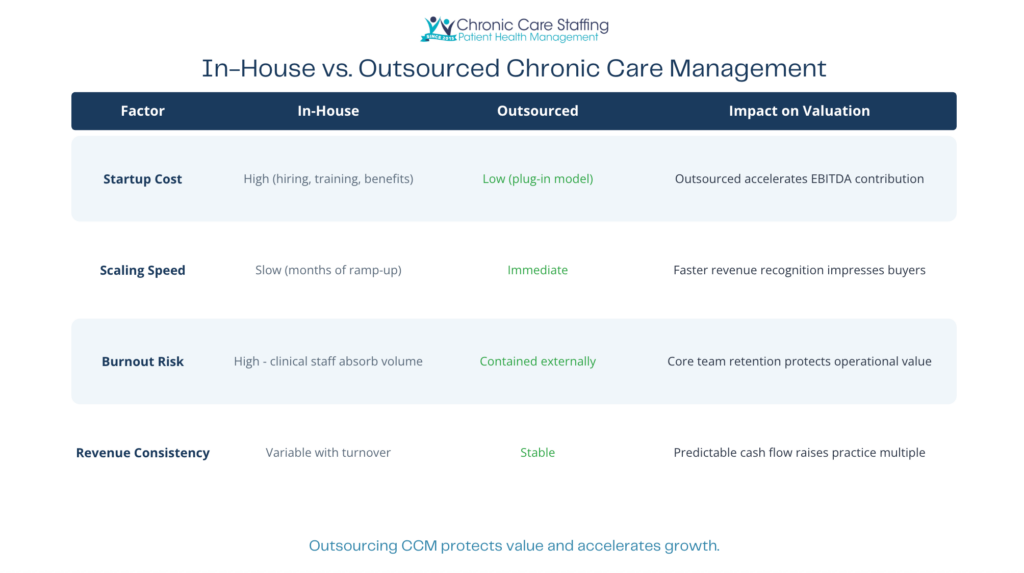
The risk of building in-house isn’t just cost — it’s fragility. A single care coordinator departure can disrupt monthly CCM billing cycles, creating the revenue volatility that due diligence specifically penalizes. Specialized staffing models eliminate that single point of failure.
In practice, outsourced care management also addresses a quieter threat: physician and staff burnout. When chronic care coordination falls to an already-stretched clinical team, quality erodes — and so does the revenue it was supposed to generate. External support preserves your core team’s capacity for higher-acuity work. Practices exploring this approach can review how a structured CCM program operates before committing internal resources.
Taken together, these operational realities tie directly into the broader financial picture — which brings the key takeaways for practice leaders into clear focus.
Care management programs are no longer a clinical nicety — they are a direct driver of practice valuation, buyer confidence, and long-term financial resilience.
As covered throughout this article, the financial and strategic case is clear. AHRQ emphasizes that measuring value in care management requires tracking both clinical outcomes and financial sustainability — and practices that master both dimensions gain a decisive edge.
Here are the four pillars every practice leader should internalize:
The strategic question, then, isn’t whether to build a care management program. It’s how to implement one in a way that maximizes your practice’s market appeal before the next valuation conversation begins.